.svg?sfvrsn=be606e78_3)
You can reduce the potential for staff diversion of opioids and patient misuse by following these steps to keep your pain medication safe and secure, from procurement straight through to disposal.
- Home
- Article
Who Has Access to Your Medications?
By: Joe Paone
Published: 1/22/2020
Share:
Reduce diversion risks with these drug security and disposal solutions.
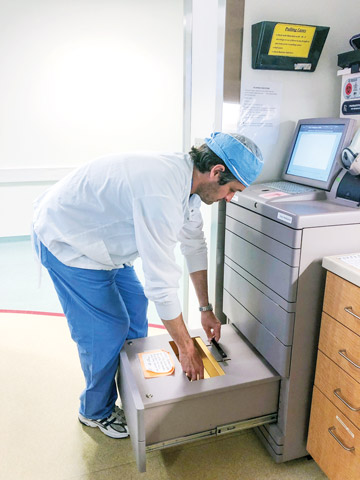
IN GOOD HANDS Automated drug storage and dispensing cabinets ensure staff obtain only the amount of medications needed for specific cases and keep digital records of usage.
| Pamela Bevelhymer, RN, BSN, CNOR
1. Regular audits
Make sure a manager — preferably someone who isn't involved in buying medications — is auditing the purchasing records of controlled drugs. "Regularly review the wholesaler account and do a line item report, looking at all drugs that were purchased and comparing them with everything that was stocked," says Kimberly New, JD, BSN, RN, founder of Diversion Specialists, a consulting firm based in Chicago, Ill. "If you don't, it's easy for a staff member to order an extra shipment of a controlled drug and take it without you ever knowing."
Also make sure separate staff members are in charge of purchasing, receiving and stocking your medication supplies, suggests Ms. New.
The careful monitoring of opioid supplies must extend into patient care areas. "One of the big issues we've seen is recovery room nurses not auditing opioid transactions," says Ms. New. "A number of cases have involved PACU nurses pulling 2 pills, but giving only 1. Nobody was auditing the actual administration records, so no one knew. The issue went unnoticed until things spiraled out of control."
2. Secure storage
Automated locking carts are the Rolls-Royce of opioid security. "It's the most secure and accountable way of managing controlled substances," says Ms. New. "You have an automated trail, so you know who's gained access to what."
Absent automation, a manually locking storage cart is the next best thing, says Ms. New. But don't lull yourself into thinking a strong lock is all you need. "I strongly recommend facilities focus a video camera on the cart that's storing controlled drugs," she adds. "And keep the key stored in a separate location, like a wall-mounted lock box, to prevent widespread access to the stored drugs."
Ms. New says it's convenient to have one central storage location for controlled substances. She's also seen some facilities that have manual locking storage cabinets pack other expensive supplies into the cabinet with controlled drugs. That's a medication security no-no. "Designated storage carts should contain only controlled drugs," she says. "Remember, you want to reduce the number of times staff members need to gain access to that location."
AT-HOME SOLUTION
Pouches Promote Safe Disposal

DON'T FLUSH Charcoal pouches deactivate opioids, making them suitable to toss in household trash.
The FDA says flushing unused opioids down the toilet is acceptable only as an option of last resort. One intriguing in-home, environmentally friendly disposal alternative: charcoal pouches. When patients place opioids in the bag and add water, the charcoal inside binds to the pills, rendering them unusable.
"We've done some studies on the use of pouches, and they definitely improve safe disposal," says Chad Brummett, MD, director of the division of pain research and director of clinical research in the department of anesthesiology at Michigan Medicine University of Michigan in Ann Arbor, and co-director of the Michigan Opioid Prescribing Engagement Network (OPEN). "I'm a big proponent of them."
His research found that the pouches doubled compliance with proper disposal directives by serving as a physical reminder to waste unused opioids in addition to the verbal and printed education patients received during their care. The pouches, which cost a few dollars each, are biodegradable and can be disposed of in regular trash.
— Joe Paone
3. Accurate counts
Perform a count of controlled drugs at both the beginning and end of every shift or day of surgery. "If you have any discrepancies or issues, you'll be able to recognize them as quickly as possible," says Ms. New.
Ms. New also stresses that 2 staff members should perform end-of-shift counts to have real-time double-checks in place. That prevents the uncomfortable situation of having to decide who's telling the truth — a manager who subsequently questions the accuracy of the count performed by a staff member working alone or the solo staff member who claims the count was correct.
Don't worry about staff pushing back on your efforts to make sure counts are correct; opioid security is always more important than hurt feelings. "Most nurses I work with welcome the additional oversight," says Ms. New. "They feel having somebody double check them is in their best benefit because if a drug is missing, they could be accused of stealing it."
4. Proper wasting
Make sure staff members work together to waste medications left over after cases. One team member should dispose of the medications under the direct observation of the other, and both staffers must document the amount of discarded drugs, and that the process was done properly and completely. Also consider adding drug disposal units that deactivate discarded medications to eliminate the possibility of staff diverting trace amounts of leftover substances.
If you're prescribing opioids, are you accounting for what happens to those opioids after patients bring them home, especially in terms of what happens to leftover medications?
Studies estimate that 75% of opioids prescribed after surgery go unused, and most of the unused medications are not disposed of properly, leaving open the possibility that a patient's relative "tries just one" when he see leftover pills in the medicine cabinets. Like many physicians earlier this decade, surgeons at Rush University Medical Center in Chicago, Ill., were prescribing opioids to patients. Furthermore, there wasn't a process in place to educate patients about how to safely get rid of extra pills.
"We weren't addressing opioid disposal at all," says Charles Hannon, MD, resident physician at Rush's department of orthopedic surgery. "If you look at the literature, an overwhelming majority of physicians and practices do not educate patients on proper opioid disposal methods."
As the national epidemic grew worse, Rush decided to take corrective action. They began with a randomized trial. Dr. Hannon and his team tested 2 patient educational methods. One involved handing patients a simple pamphlet, which described FDA-approved opioid disposal methods, such as bringing them to medication takeback boxes at local pharmacies, hospitals, and fire and police stations or, failing that, flushing them down the toilet. The team gave each patient the pamphlet on 3 occasions: pre-operatively, 3 weeks post-op and 6 weeks post-op. The second method consisted of giving patients the same pamphlet, but and also sending them text message reminders about proper disposal methods.
The result? About 38% of the text/pamphlet group disposed of their pills properly, while about 33% of those with just the pamphlet did. Of course, that means 3 out of 5 patients did not dispose of their opioids properly. But that rate is better than patients who received no education at all — the study showed less than 10% of these patients followed proper disposal protocols.
Dr. Hannon suggests you provide educational materials about opioid disposal to surgeons, who can then pass the information along to their patients. He adds that it's important for patients to be educated more than once and through different methods — pre-operatively, post-operatively, and through post-op calls or texts.
"At the end of the day, we're probably not where we need to be in terms of the percentage of patients who actually are properly disposing of their pills," says Dr. Hannon. "But I think if you're able to raise the baseline rate of opioid disposal from 10% to 35%, that's a huge deal. If you're able to prevent at least one diversion of an opioid pill and prevent one life lost, that's a job well done." OSM
3. Accurate counts
Perform a count of controlled drugs at both the beginning and end of every shift or day of surgery. "If you have any discrepancies or issues, you'll be able to recognize them as quickly as possible," says Ms. New.
Ms. New also stresses that 2 staff members should perform end-of-shift counts to have real-time double-checks in place. That prevents the uncomfortable situation of having to decide who's telling the truth — a manager who subsequently questions the accuracy of the count performed by a staff member working alone or the solo staff member who claims the count was correct.
Don't worry about staff pushing back on your efforts to make sure counts are correct; opioid security is always more important than hurt feelings. "Most nurses I work with welcome the additional oversight," says Ms. New. "They feel having somebody double check them is in their best benefit because if a drug is missing, they could be accused of stealing it."
4. Proper wasting
.svg?sfvrsn=56b2f850_5)