.svg?sfvrsn=be606e78_3)
One GI group is finding out in real-time.
 Ohio Gastroenterology Group
Ohio Gastroenterology Group AT YOUR SERVICE Ohio Gastroenterology Group is leveraging artificial intelligence to improve and enhance communications with patients while freeing human staff to have more meaningful interactions in person and over the phone.
When Ohio Gastroenterology Group, a Columbus-based physician-owned practice with five endoscopy centers, was drowning in tens of thousands of monthly phone calls after the pandemic, its leaders turned to artificial intelligence (AI) for help.
“It was impossible to have enough people to answer every call in a timely manner,” says gastroenterologist and board member Raghuram Reddy, MD. “Lots of voicemails means upset patients, so we had to find solutions.”
Forward-thinking practices over the last decade have gradually implemented text messaging, email and smartphone apps for patient communication, while providing richer information on their websites. Some offer web-based portals through which patients can securely access personal records, providers and other information. Ohio Gastroenterology wants to avoid the weaknesses of these approaches that still frustrate some patients by taking it even further — to provide something more seamless, personalized and easier to use for both the practice and the patient.
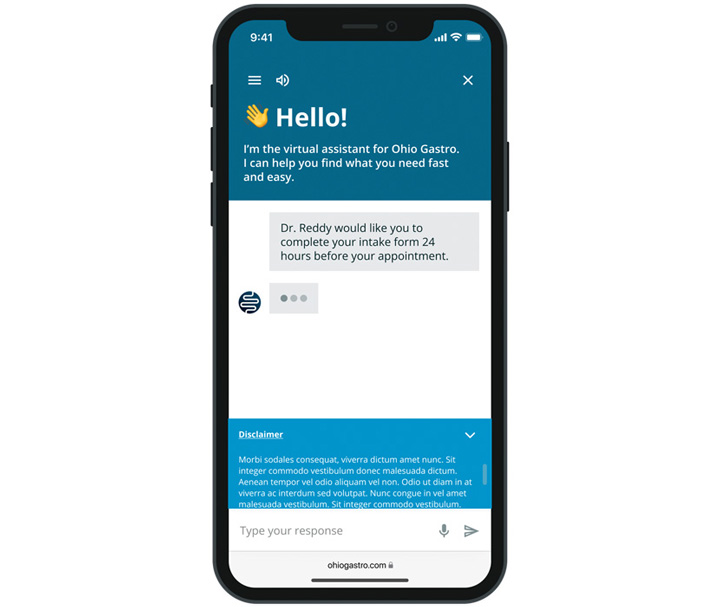
It’s doing this via a highly configurable, private and secure patient communications platform that enables providers to develop and implement “smart virtual assistants” powered by conversational AI via web, text and voice. The platform automates communication workflows that humans such as overburdened doctors, nurses and staff previously needed to perform. Dr. Reddy says the platform furthers his vision of providing “directed self-service” to patients.
Last year, Ohio Gastroenterology launched the platform by providing self-serve access to COVID-19 information, insurance coverage and billing processes. To support intake workflows, it later launched automated outreach programs in which interactive virtual assistants deliver pre-op instructions and post-op check-ins. This year, it will implement referral scheduling functionality that enables patients to book recommended appointments digitally.
The practice anticipates self-scheduling will reduce leakage and capture revenue from patients who otherwise might not have scheduled. Still to come is a visual patient assessment tool whose range of images will allow patients to share detailed information about where they are experiencing pain.
Dr. Reddy says Ohio Gastro is simply catching up with how patients interact with almost everything else in life by being available virtually 24/7/365. “You can fly all around the world without talking to anyone, but in most cases, you cannot schedule a colonoscopy or endoscopy without speaking with a human,” he says. The intent is not to eliminate human interactions, but to optimize them. If a patient would prefer to speak to a live human being, that option is always available.
The practice and the platform’s vendor continuously monitor the system to ensure patient satisfaction. “The statistics it generates will tell us if people are getting frustrated, so we’ll know if we need to make changes,” says Dr. Reddy. But it does require significant work on his end to maximize the platform’s capabilities and achieve his vision of directed self-service.
“I want my patients to hear what I think is appropriate, as opposed to whatever is out there on Google,” he says. “All of this takes some intelligence in the background. We made a bank of hundreds of questions where patients can chat and interact with the AI with answers vetted and curated by us, so I know they get the right answers. We provide all the clinical content; the intelligence happens in the background.”
Dr. Reddy estimates the system’s automation of routine workflows can save 45 minutes per provider per day, allowing the practice to see more patients and potentially realize a seven-figure increase in annual revenue.

.svg?sfvrsn=56b2f850_5)