.svg?sfvrsn=be606e78_3)
- Home
- The Magazine
- Article
Murder in Memphis
By: Outpatient Surgery Editors
Published: 10/4/2023
Share:
Dr. Ben Mauck’s killing has industry insiders worried about what can be done to keep healthcare workers safe on the job.
When Benjamin M. Mauck, MD, was fatally gunned down in a Collierville, Tenn., exam room in July, allegedly by a troubled patient, the Memphis-area community lost more than a talented pediatric orthopedic surgeon. By all accounts, the popular Dr. Mauck was also an amazing father, husband, colleague and friend.
The killing of Dr. Mauck by one of the people he was trying to treat is part of a troubling trend that puts healthcare workers’ lives in danger simply by being on the job seeing patients each day.
Multiple studies show that violence against doctors, nurses and other healthcare workers seems to be on the rise. Healthcare workers’ risk of injury due to workplace violence is five times greater than employees in other industries, according to the U.S. Bureau of Labor Statistics. Nurses are especially vulnerable to this issue, according to a 2022 study from National Nurses United that found 40% of nurses had seen an increase in violence.
No single factor is driving the surge in violence, and ASCs could be more prone to these sorts of attacks.
“Many ambulatory centers are designed to be accommodating and welcoming to the public and have limited physical barriers in place to protect the staff,” says Andy Poole, FACHE, associate director of strategy and innovation at ECRI, an independent nonprofit organization with global headquarters in Plymouth Meeting, Pa. “Centers need to be constantly evaluating the actions they can take to protect their team. When employees do not feel safe, it will lead to increased stress and burnout, continuing the cycle of staff turnover which we know contributes to greater risk of accidental harm.”
In addition to the obvious peril to the workers themselves, the prospect of violence at healthcare facilities makes it more difficult and expensive to care for patients.
In an attempt to ensure worker safety, some agencies are calling for violence-prevention measures that range from metal detection at entrances, to teaching healthcare workers to identify signs of imminent trouble and what to do if an incident begins, to creating new laws specific to assaults against medical workers.
Dr. Mauck’s murder is a chilling example of how vulnerable healthcare workers are to a worst-case scenario. Those who loved him have grieved his death and paid tribute to his life. He was laid to rest in a Catholic church one morning in July, hours before Larry Pickens, the 29-year-old Memphis man accused of the killing, appeared in court.
Irina Ollar, spokesperson for Campbell Clinic Orthopaedics, where Dr. Mauck was killed, called his death “a tragic loss” and said he was “one of our highly respected and beloved physicians,” in a statement shortly after the shooting. “We ask that you lift his family in prayer.”
Dr. Mauck’s commitment to children was evident in a TV appearance on a Memphis news station about fireworks safety just days before he was shot. The elbow, wrist and hand surgeon was a treasured member of the community of Collierville, the site of a 2021 mass shooting at a grocery store during which one person was killed and 13 were injured. He had been at the Campbell Clinic since 2012 and was a 2006 graduate of the University of Tennessee-Memphis Medical School, and in June was named one of the Top 2023 Doctors in Memphis by the Castle Connolly medical group.
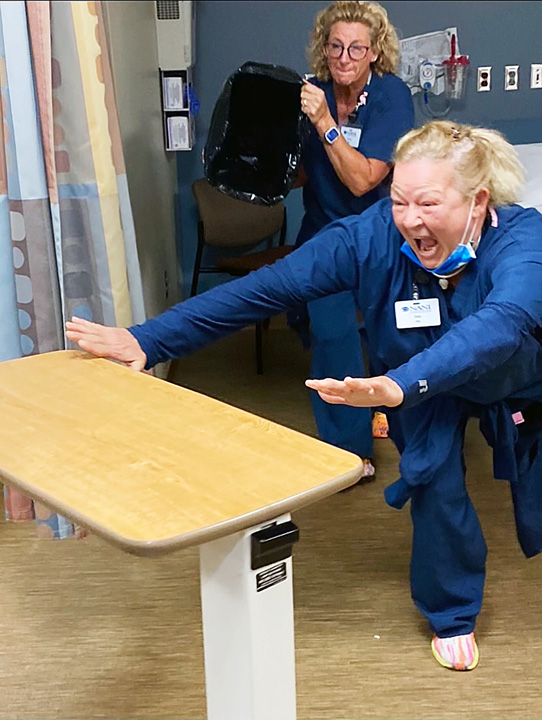
READY FOR ANYTHING NANI Vascular incorporated more realistic active-shooter drills into its regular training following a rise in shootings at healthcare facilities.
Mr. Pickens was charged with first-degree murder and aggravated assault and his bail was set at $1.2 million. He was in Collierville Municipal Court on Aug. 29, but the session was continued when it was learned that his mental health evaluation was incomplete, according to the court’s Chief Clerk Patrick Lafferty. His next court date is scheduled for Oct. 24. The case will eventually be sent to the Shelby County Grand Jury for a potential indictment on the charges, says Mr. Lafferty. Outpatient Surgery Magazine contacted Mr. Pickens’ court-appointed attorney John Dolan for comment. For now, the case against Mr. Pickens is as murky as the path forward to making America’s hospitals, clinics, surgery centers and other facilities safer places.
Police have said that Mr. Pickens was involved in some type of conflict at the Campbell Clinic about a week before the shooting and had been a patient of Dr. Mauck’s for approximately two years. The gun used in the attack was legally purchased by Mr. Pickens on July 3. Collierville Police Chief Dale Lane says the patient was at the clinic for several hours before the shooting and believes it was a targeted attack, a contention bolstered by the fact that no one else in the office or the building was shot. Mr. Pickens was arrested outside the clinic within five minutes of police arrival without incident.
Even though the incident doesn’t appear to have been an intended mass shooting, Chief Lane noted that the clinic staff performed admirably under a stressful situation, making sure staff and patients were accounted for and having Mr. Pickens’ name and description ready for officers when they arrived. “They were practicing what they had been trained for in active shooter training. That absolutely makes a difference,” says Chief Lane. “I commend the folks at Campbell Clinic who made sure the employees were trained.”
On the heels of another tragedy
In March 2022, the American Academy of Orthopaedic Surgeons (AAOS) launched a Work Environment and Culture Survey to better quantify and understand the level of verbal abuse, threats and assaults its membership was experiencing, as well as the safety of its members’ current work environments.
The results were distressing. In the previous 12 months, 40% of respondents had experienced some type of workplace violence and 30% had experienced physical threats. The survey found 54% of respondents were at least moderately concerned about workplace violence and thought about it with some regularity, while 72% had experienced verbal abuse. Additionally, 25% of the physical threats and 16% of the physical assaults involved a firearm and/or some other type of weapon.
“These were fairly surprising statistics, with a large percentage of respondents having experienced workplace violence, and several respondents encountering actual physical assaults,” says Julie B. Samora, MD, PhD, MPH, FAAOS, an orthopedic surgeon with Nationwide Children’s Hospital in Columbus, Ohio, who chairs the AAOS committee on healthcare safety.
The June 2022 murder of spine surgeon Preston Phillips, MD, on the campus of Saint Francis Health System in Tulsa, Okla., which occurred while the AAOS survey was in process, appears to have been an inflection point among orthopedic surgeons in terms of personal awareness about the potential for violence in their workplaces.
“We found that the majority of our survey respondents reported little to no concern about workplace violence prior to the Tulsa incident,” says Dr. Samora. “In contrast, after the Tulsa incident, the majority of respondents reported that they did have concerns on a regular basis.”
Dr. Samora says the survey found that verbal abuse was by far the most commonly reported form of workplace violence among orthopedic surgeons when compared to verbal threats, physical threats and physical assaults. She says the most at-risk orthopedic subspecialists are trauma surgeons and tumor surgeons.
Dr. Samora notes that workplace violence incidents in the broader world of health care increased by 57% from 2013 to 2020, according to research from the U.S. Bureau of Labor Statistics. “Historically, there have always been threats, but violence is on the rise everywhere,” she says. “It is unclear why this rise in violence is occurring, but it likely can be attributed due to complex multifactorial socioeconomic and cultural reasons,” she says.
The best approach for violence prevention is to be proactive rather than reactive, says Dr. Samora. “Staff training, enhanced security checkpoints, physical barriers and increased patient screening enable a prepared response to facilitate action in an emergency situation,” she says. “If a business is situated in an environment with a history of violent crime, increased security should be implemented — for example, locked doors, having viewing windows or cameras and having the ability to ask questions of a potential perpetrator before they are allowed access. Establishing heavy iron or metal barriers can provide staff a safe haven to drop and cover.”
Dr. Samora says perpetrators of workplace violence often have had prior involvement with the facility or provider. “If there has been any previous risky situations, it should be communicated to the entire staff to increase heightened awareness,” she says, adding that significant threats should be reported to local authorities.
“Several institutions have created flags for patients at high risk for violence,” adds Dr. Samora. “In our institution, we have embedded within our electronic medical record a purple banner for patients that have displayed violent behaviors in the past. It is immediately visible upon opening the patient chart. This allows for early recognition and preparation for potential threatening situations.”
Dr. Samora says certain security ideas simply aren’t workable options for surgical facilities. “Screening X-ray machines have significant costs associated with them, could potentially alienate our patients and families and may not actually prevent someone from doing harm, as perpetrators could go around the detector,” she says. “Secured dual-door systems can be useful but perhaps more burdensome as one extra step for staff. Patting patients down can be very affronting and could negatively impact the doctor/patient relationship.” Dr. Samora says many relevant training programs exist:
• CRASE (Citizen Response to Active Shooter Events) training preemptively prepares staff for an appropriate response prior to an active shooter event.
• AVADE (Awareness-Vigilance-Avoidance-Defense-Escape) educates employees on how to avoid, deescalate or defend themselves in threatening situations.
• SAVE (Security Awareness and Vigilance for Everyone) is a program at Massachusetts General Hospital that teaches employees how to recognize and report suspicious individuals.
• Armed Intruder Training, a model developed by the U.S. Department of Homeland Security, lays out what employees should do when an armed intruder enters the facility.
“De-escalation techniques can be taught as well,” says Dr. Samora. “If rapport with the perpetrator can be gained, it is less likely that harm will occur.”
This May, AAOS launched its own Workplace Violence Toolkit (available at aaos.org/toolkits). “This toolkit aims to educate users about the prevalence and various forms of workplace violence, as well as how to recognize warning signs, implement preventive measures and outline steps to take before, during and after an incident,” says Dr. Samora. “Notably, the Workplace Violence Toolkit has been accessed two to three times more frequently than any other toolkit available on the AAOS website.”
Regardless of whether employees have received training, if a threat is recognized or a confrontational or violent interaction occurs, police and security should be contacted immediately. Dr. Samora notes that some states require healthcare facilities to have workplace violence prevention plans in place, and that The Joint Commission is considering requirements for workplace violence prevention.
Dr. Samora says AAOS pushed for passage of the federal Safety from Violence for Healthcare Employees (SAVE) Act, which would provide healthcare workers protections from assault and intimidation similar to those provided for Transportation Security Administration workers and flight crews. Workplace violence was a focus of AAOS’ 2023 Orthopaedic Advocacy Week in July, and AAOS leadership has discussed collaborative efforts with leaders from the American College of Surgeons (ACS) and the Orthopaedic Trauma Association to take steps to protect their members and their patients.
AAOS also has aligned with the ACS’ Firearm Strategy Team workgroup (osmag.net/FAST).
Realistic training, extra precautions

TAKE COVER NANI Vascular staff practice ducking behind a stretcher during one of the facility’s recent active shooter training sessions.
While facility leaders watch for legislation like the SAVE Act to pass, the sad reality is they still must prepare staff to protect themselves from violence now. For many, that means more regular and realistic active shooter training. That’s why Cynthia Wiersema, RN, BSN, director of nursing at NANI Vascular in Fort Wayne, Ind., recently decided to incorporate Nerf guns into the facility’s annual active shooter training. “The decision stemmed from the unfortunate increase in active shooter incidents across various settings,” says Ms. Wiersema.
Ms. Wiersema says that prior to her 2020 arrival at the surgery center, which specializes in outpatient procedures for dialysis patients, staff would watch active shooter videos and take a short quiz at the end. “This didn’t give them the experience that they needed to be successful in emergency situations. We firmly believe that hands-on training holds more value than solely relying on videos and walkthroughs.”
The training is unannounced to her small eight-member staff. It begins by recruiting one of her nurses to play the role of the active shooter. “The recruited nurse will walk through the front door and ‘open fire’ her Nerf gun at the receptionist,” says Ms. Wiersema. The receptionist will then hit the alarm, which alerts the staff that an active shooter is on the premises. “At that point in time, staff need to identify which strategy they are going to take.” By simulating real-life scenarios, her staff gains a genuine understanding of the limited time they have to react and respond.
While the actual shooter training has been invaluable, Ms. Wiersema says the post-drill discussions are equally as significant.
“Staff members discuss multiple areas where they can hide and barricade themselves effectively,” she says. “Additionally, we educate them about various objects within those rooms that can be utilized as makeshift weapons — such as scissors, for example — should the need arise.
“By encouraging staff members to contribute their perspectives and suggestions, we create an environment where everyone can learn from one another and collectively improve their response strategies,” she says.
Ms. Wiersema says healthcare workers instinctively want to help others, but in an active shooter situation, that instinct can be dangerous. “We must first ensure our own safety before we can provide care to others,” she says. “We believe that this approach not only prepares our staff for the worst-case scenario, but also promotes a culture of safety and self-preservation. We cannot be of service to anyone if we are injured or dead ourselves. We also feel that it is important to share our methods with others in the healthcare community and hope it inspires others to consider new and innovative ways to prepare for such situations.”
Mr. Poole, the director from ECRI, noted that the ASC he used to work at in Virginia had local police come in and do an assessment of physical barriers, response readiness and potential risks. He says he has mixed feelings about the prospect of metal detectors at the front doors of such facilities. “I feel metal detectors won’t do much and will only make a difference if you have the right policies, training and personnel to respond appropriately,” he says. OSM
.svg?sfvrsn=56b2f850_5)